
Dynamic Navigation In Cases Of Critical Anatomy
Dr. David Burguess (United Kingdom, 2017)
Dynamic Navigation For Precise Implantation In Cases Of Critical Anatomy
INTRODUCTION
Using the CBCT image as a map, dynamic navigation guides surgeons just like a GPS guides drivers. The clinician virtually plans where implants should be placed. During surgery, the navigation system dynamically tracks the drill and the patient’s jaw, providing guidance and visual feedback to ensure the implants are placed according to plan.
There are several advantages with dynamic navigation. The technology allows clinicians to place implants more accurately than free-hand. This results in improved safety and aesthetics, as it helps the clinician to anticipate and to avoid potential complications. Other advantages are the ability to have more minimal invasive treatments, which means less chair time, less patient discomfort and less recovery time. This treatment option has generally been seen as a ‘blind’ procedure in the past, but the ability to avoid delicate anatomical structures due to the real-time surgical feedback makes so-called flapless surgery a valuable option.
In the following case report, Dr David Burgess describes how using computer-guided dynamic navigation helped him overcome clinical challenges for dental implant placement in the lower posterior region.
Case Report
A 75-year-old male patient had endured a gap for five years, following removal of his lower left second molar, due to an acute apical infection. He was finding mastication increasingly difficult and sought advice about the treatment options available.
Planning for optimum implant positioning
As there was no tooth distal to the space, conventional fixed bridgework was not possible. The treatment options were either a unilateral single saddle lower partial denture or restoration of the space with two dental implants. The patient chose to have dental implant treatment as he did not wish to have any form of removable prosthesis.
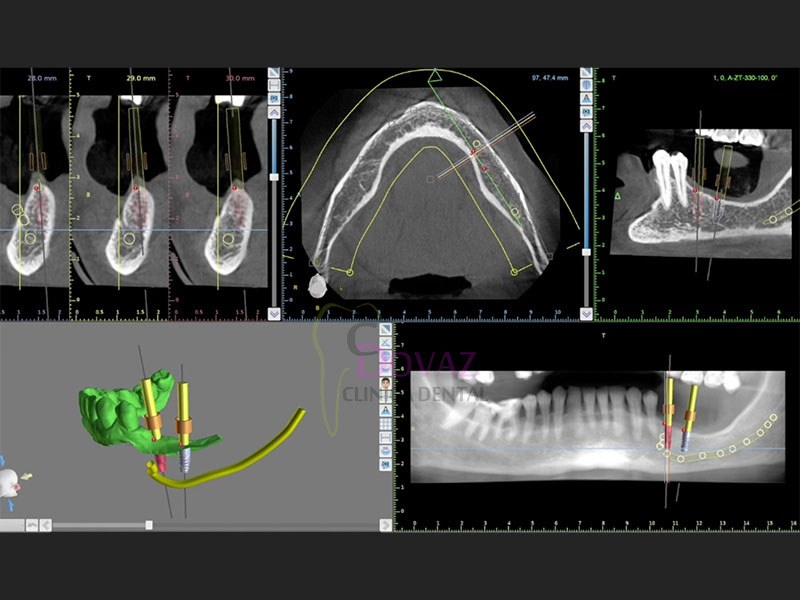
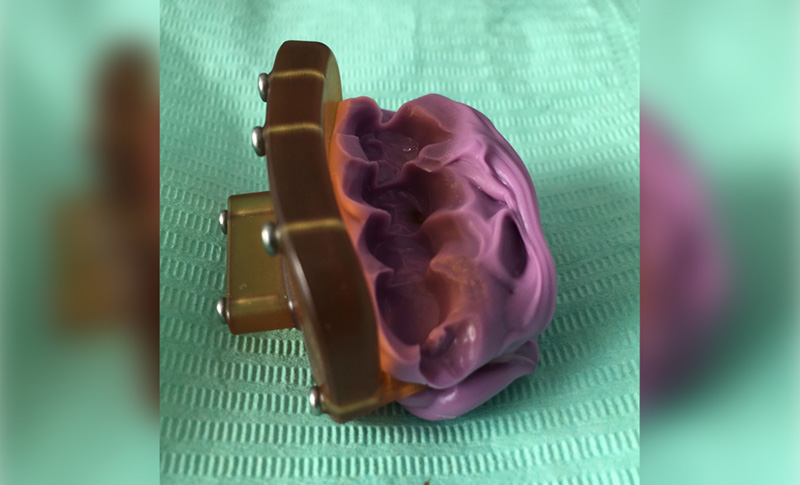
What makes Navident dynamic navigation stand out is it precisely guides the surgeon to prepare and place the implant in a pre-determined position (Figure 1). This allows me to achieve greater accuracy and certainty than I have previously been able to, using conventional protocols. Whilst there is no physical guide, a simple scanning template (NaviStent) is used to hold the fiducial in place whilst taking the CT scan, and secure the jaw reference (JawTag) for the navigated osteotomy.
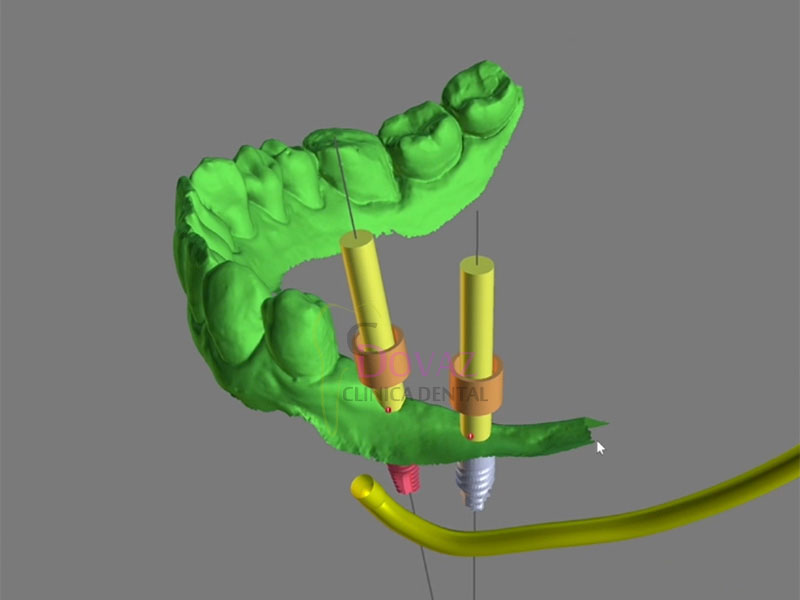
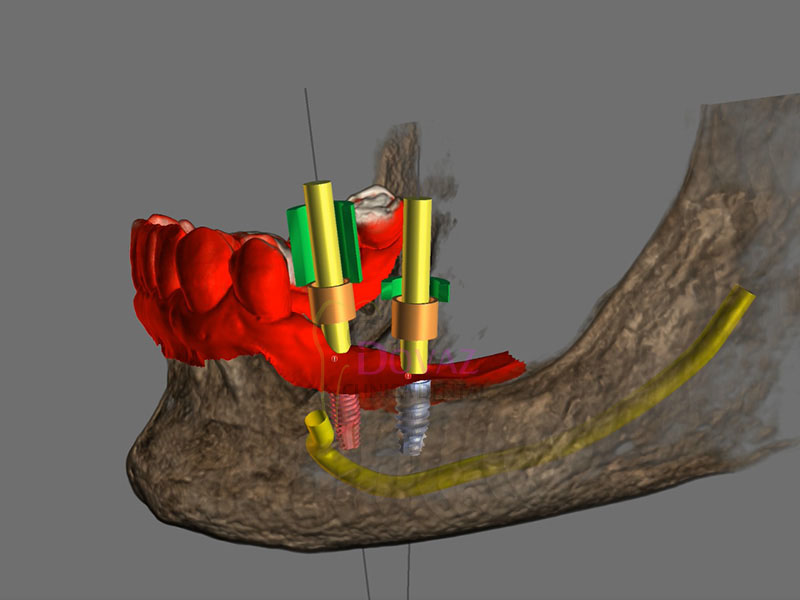
In this case, the Navistent was fabricated, the fiducial marker attached and a CBCT scan taken two weeks prior to surgery (Figure 2). The treatment plan was created immediately after the scan (Figure 3), with the patient present. He was able to see the proposed treatment displayed by the Navident software and appreciated that great care was being taken to achieve the optimum implant positioning, with minimal risk of potential complications (Figure 4). The patient was extremely impressed with, and reassured by, the state-of-the-art technology.
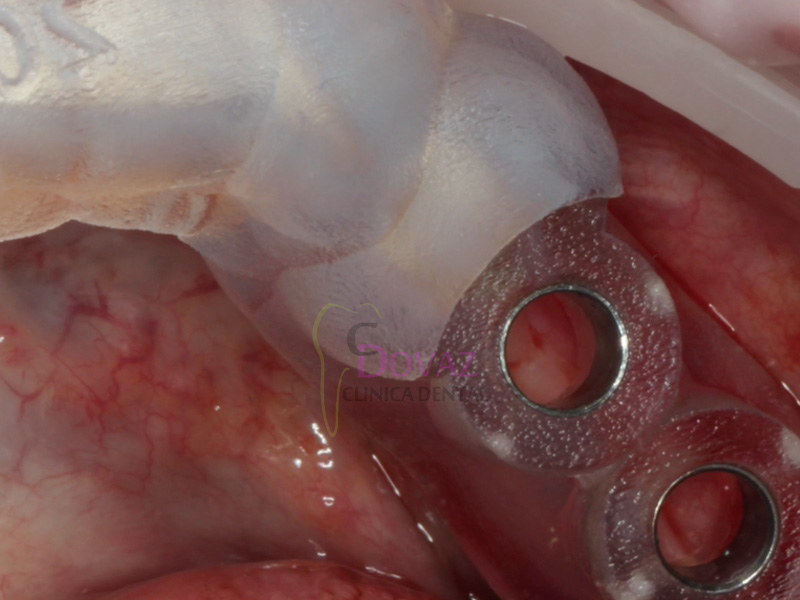
Confidence from continuous feedback Treatment was carried out under local anaesthesia. Prior to preparation of the implant sites, the simple Navident protocol for calibration and verification of the drill axis and drill tip was carried out. A crestal incision was made, with a minimal flap reflected. The software shows the drill position on the scan in real time, as it enters the jaw. This allows adjustments to be made, if necessary, whilst the site is being drilled. Two DENTSPLY ANKYLOS® CX 3.5mm diameter dental implants were placed sub-crestally in the lower left first and second molar sites, with implant lengths of 11mm and 9.5mm respectively.
Avoiding damage to the inferior alveolar nerve was a crucial factor in the treatment planning of this case. Access was difficult, due to the limited opening of the patient’s mouth. The issue was compounded by the plan to place an implant as distal as the second molar. These challenges were overcome using Navident’s continuous internal visual feedback, which gave me the confidence to use the optimum length of implant, whilst staying within a safe distance from the inferior alveolar nerve and avoiding post-surgical complications, such as paraesthesia.
Navident provided guidance for accurate implant location, even with restricted visibility and the drill being impeded by opposing teeth. Tactile feedback can often be reduced when using a physical drill guide. Dynamic navigation removes this obstacle. I was able to achieve the best buccal and lingual position of the implants, and their relation to each other and to adjacent teeth (Figure 5). This would allow for optimal shape, position and occlusal function of the final restorations.
ANKYLOS® Balance posterior sulcus formers were fitted and the incision was closed with simple interrupted sutures. There was no need for bone augmentation. Two to three months after surgery, the implants will be restored with ATLANTIS® custom-made CAD/CAM titanium abutments and screw-retained linked zirconia crowns.
The clinical outcome was excellent. The planned placement was restoratively driven and the implants were well positioned, with good primary stability. Having used the Navident dynamic navigation system for more than a year, I would not want to go back to preparing and placing dental implants without its 3D visual guidance. The patient was comfortable and reassured, with no post-operative pain, swelling, bruising or paraesthesia. He was delighted and, if he needed any implant treatment in the future, would insist on dynamic navigation.
About Dr David Burgess BDS DPDS MScConSed
David Burgess has been principal of Carbis Bay Dental Care in Cornwall since 1988 and has placed over 2,000 implants. Throughout his career, David has striven to combine clinical perfection with the ultimate in patient care. He has been a willing pioneer of new technology, particularly in the field of digital dentistry. David was the first UK clinician to introduce the Navident dynamic navigation system into his implant treatment workflow, with the objective of achieving a higher degree of precision and greater patient comfort.
David Burgess is also a member of the Dynamic Navigation Society as a Master Clinical Trainer, providing courses for implantologists who wish to experience how dynamic navigation can help to simplify their digital workflow. More information can be found on http://dns.claronav.com





Dr David Burgess
Carbis Bay Dental Care
6-7 Boskerris Terrace
St Ives Road
Carbis Bay
St Ives
Cornwall TR26 2SF
Tel: 01736 793090
Email: [email protected]
www.carbisbaydental.co.uk
Dynamic Navigation by innovative registration
Dr. Ricardo Henriques (Portugal, 2018)
Dynamic Navigation By Innovative Registration.
Background
3-D implant planning and mapping that plan to the real surgical environment are two important steps in implant rehabilitation.1,2 Misplaced implants can create difficult aesthetics, functional and biological problems and can result in implant loss.3–5
There are three ways to transfer a planned implant’s position into the real patient’s jawbone:
- mental navigation, so-called freehand navigation,
- static navigation using surgical templates,6 and
- dynamic navigation using a stereoscopic camera.7,8
The freehand approach is totally dependent on the surgeons’ experience, skills and mindset during treatment and creates the highest deviations compared to the other approaches.2
The usage of surgical templates provides a higher accuracy compared to freehand surgery, but has a few limitations, such as the inability to modify the plan once the surgical template has been manufactured. Surgical templates require longer drills which can make their use quite difficult or even impossible. Other concerns are irrigation issues and incompatibility with advanced surgical protocols.
Dynamic navigation is, at present, the most effective way to transfer the planned implant’s position to the real patient as it guides the surgeons’ motions using real-time feedback. It is especially useful to reduce flapped procedures with the advantage of improved soft-tissue healing, patient comfort and reduced bone resorption. Dynamic navigation allows planning modifications at any time, even during treatment, and can be used in cases with limited mouth opening or in combination with osseodensification drills.
The dynamic navigation concept using trace registration
In this approach, the patient’s jaw and the surgical drill’s location are being tracked by the navigation system’s tracking camera, using special tags affixed to them. To correspond between the physical patient’s jaw and its on-screen cone beam computed tomography (CBCT) scan representation, the tag installed on the patient’s jaw must be mapped with the CBCT scan. The mapping of the trackable jaw tag to the CBCT scan is called registration. Traditionally, the patient would have to be CT-scanned with an artificial radiographic marker, also known as “fiducial”, which has to be later identified in the CT images by the navigation system’s software in order to enable the registration.7
The innovative trace registration method (Navident, ClaroNav) eliminates the need for this artificial fiducial body to be present in the image, by replacing it with natural high-contrast surfaces, such as tooth crowns or abutments already present in the image. Therefore, it eliminates the need for patient exposure to a new dedicated CT scan with a fiducial. The level of radiation is an important issue in diagnosis.9,10 This new method also eliminates the need to have a special stent prepared to couple the fiducial or trackable tag to the jaw in a highly stable and repeatable manner, which was previously essential for the performance of accurate navigation.
To treat the maxilla, a pattern tag, or Head-Tracker, is positioned on the patient’s head like glasses with contact points that don’t move with patient muscle contractions or lower jaw movement (Fig. 1). This ensures that the Head-Tracker maintains a stable relationship with the skull, and thus the maxilla. For the mandible, another pattern tag, called Jaw-Tracker, is temporarily connected to one to two teeth using dual-cure composite resin (without etching the teeth to allow for easy removal; Fig. 2). This Jaw-Tracker can also be used for the maxilla instead of the Head-Tracker.
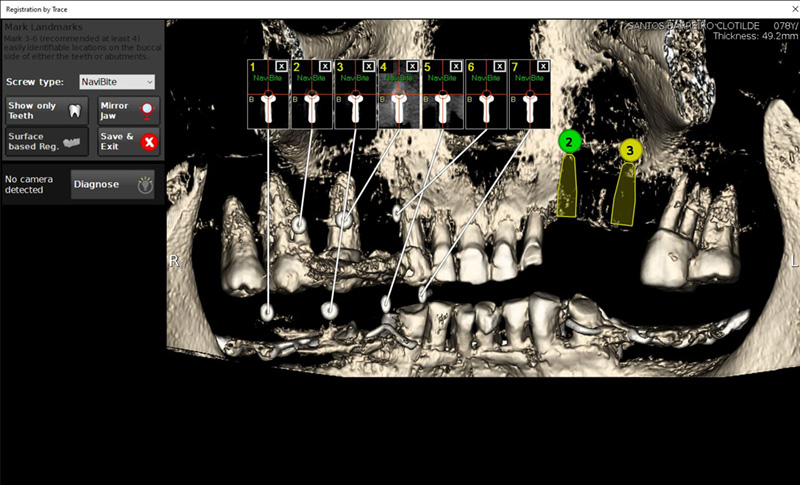
The surgeon chooses four to six identifiable landmarks on structures which are rigidly attached to the jawbone (teeth, abutments) and are easily visible in the CBCT scan. In the next step, the surgeon traces a path on the surface of each one of the marked structures with a tracer tool, also tracked by the camera (Fig. 3). The system collects 100 points on each one of the traced structures, and optimally matches them to the CT image data to register the Head-Tracker or Jaw-Tracker, with the patient’s maxillary or mandibular CBCT scan, respectively.
Advantages of trace registration
The most important advantages of the trace based over the fiducial/stent-based registration method are:
- No need to design and fabricate a stent or guide in advance, eliminating the associated preparation time and effort, as well as the potential risk for inaccuracy due to improper seating of the stent during the scan or procedure.
- An existing CBCT scan can be used, there is no need for a special scan with stent and fiducial(s). The scan may be taken in full occlusion resulting in easier digital prosthetic planning.
- No stent or guide is in the patients’ mouth during treatment, allowing the same access space in the oral cavity during surgery as with a freehand approach.


Possible limitations
- At least four high-contrast structures fixed to the jaw bone must be available and accessible for tracing. These can be teeth, abutments, bone screws, orthodontic brackets and wires, or similar structures. With fully edentulous patients, regions of the jaw bone itself may be exposed and used as landmark regions.
- Each of the traced regions should not have changed in appearance or location relative to the jaw bone since the scan was taken. If guidance is critical and changes to the jaw such as changes in teeth position are a concern, a fresh scan prior to surgery is advised.
Case presentation
The treated patient was a 54-year-old female with a removable prosthesis, who wished to have a fixed solution. The patient was a non-smoker without medical problems. Intraoral examination revealed the absence of tooth #24 and bone resorption where the teeth had been extracted.
Planning procedure
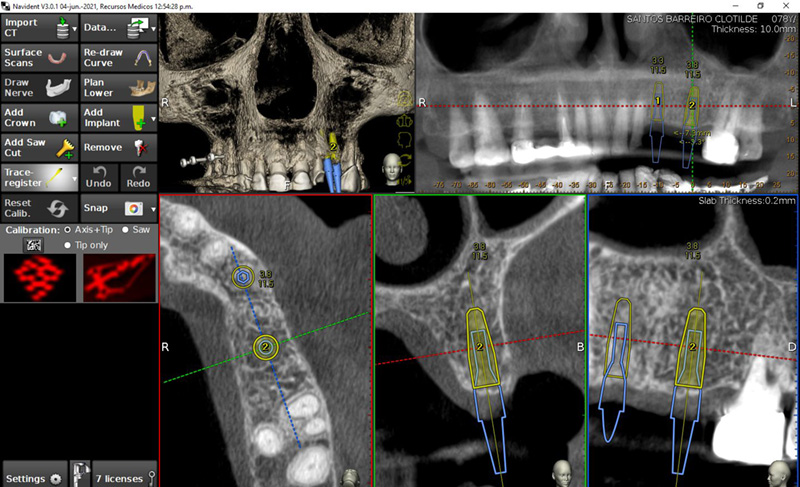
A CBCT scan was taken without any radiographic marker (Fig. 4). The images were taken with a Carestream 8100 3D (Henry Schein). The field of view used was 80 x 90mm and a voxel size of 150μm. The exposition parameters were 84kV and 4mA. The images were analysed and converted into DICOM files and then converted into a 3-D virtual model by the Navident software. A virtual crown and implant were planned to have 2mm of buccal bone and a restorative space at the centre of the crown (Fig. 5). The virtual implant planning was then modified creating an angulation of six degrees in vestibular direction, so the surgeon would be guided to initiate bone preparation with a six-degree vestibular angulation (Fig. 6).
Surgical procedure
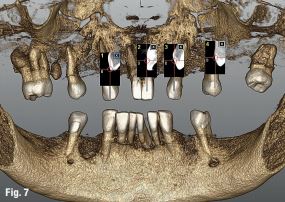
Local anaesthesia was performed in region #24 and aseptic and sterile conditions were applied to prevent infections. The Head-Tracker was positioned and inspected for stability. Trace registration was performed by marking four landmarks on teeth using a panoramic 3-D presentation of the jaw, then tracing the landmark regions with the tracer tool while the camera and software collected 100 points on each tooth (Fig. 7). Navident automatically registered the Head-Tracker with the patient’s maxillary CBCT scan based on the collected points.
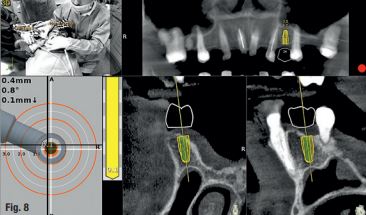
In the next step, drill calibration and accuracy check were performed before the use of each drill. A small incision for a reduced flap was made. All osteotomies were performed at 800 rpm. The virtual implant angulation was pre-surgically modified six degrees in vestibular direction, so the osteotomy could be initiated on that angle. Next, the virtual implant was repositioned intraoperatively on the Navident software and the rest of the site preparation was carried out according to the final angulation with osseodensification drills (Fig. 8). The osteotomies were made with two angulations and tracked in real time and the same procedure was applied for the implant insertion. A cover screw was attached before the surgical area was sutured. The patient reported no discomfort during the surgery.
Postoperative evaluation
The patient reported no pain or swelling. Radiographic and clinical images were taken with a direction indicator screwed onto the implant. The postoperative evaluation showed that the position of the implant exactly corresponded to the virtual planning made beforehand (Figs. 9–14).
Conclusion
The patient benefited from a treatment with a reduced flap and precise implant placement using dynamic navigation technology with an innovative trace registration method. Trace registration in combination with dynamic navigation proved to be a valid technology for osteotomy preparations and implant placement. It does not require a dedicated CT with a radiographic marker nor the fabrication of a stent or clip. When clips or stents are difficult or impossible to use, or even in every dental patient case, trace registration can be the best solution for dynamic navigation implant placement.









References
1. Somogyi-Ganss E, Holmes HI, Jokstad A. Accuracy of a novel prototype dynamic computer-assisted surgery system. Clin Oral Implants Res. 2015 Aug;26(8):882-90.doi: 10.1111/clr.12414.
2. Block MS, Emery RW, Lank K, Ryan J. Implant Placement Accuracy Using Dynamic Navigation. Int J Oral Maxillofac Implants Surg. 2017; 75:1377-1386.
3. Umapathhy T, Jayam C, Anila BS. Overview of surgical guides for implant therapy. Journal of Dental Implants, 2015 Jan-Jun; 5(1):48-52.
4. Kate MA, Plaskar S, Kappor P. Implant failure: A dentist’s nightmare. J Dent Implant 2016; 6:51-56.
5. Palma-Carrió C, Maestre-Ferrin l, Peñarrocha-Oltra D, Peñarrocha-Dago MA, Peñarrocha-Diago M. Risk factors associated with early failure of dental implants. A literature review. Med Oral Patol Oral Cir Bucal. 2011 Jul; 16(4):514-517.
6. Borisov R. Radiological templates and CAD/CAM surgical guides. A literature review. J of IMAB. 2016 Jul-Sep; 22(3):1285-1295.
7. D’ahese J, Ackhurst J. Bruyn H. Immediate loading with dynamic navigation implant surgery. International magazine of oral implantology. 2015; 3:34-37.
8. D’haese J, Van De Velde T, Komiyama A, Hultin M, De Bruyn H. Accuracy and Complications Using Computer-Designed Stereolithographic Surgical Guides for Oral Rehabilitation by Means of Dental Implants: A Review of the Literature. Cl in Impl Dent Rel Res 2012; 14:321–335.
9. Dula K, Mini R, van der Stelt PF, Buser D. The Radiographic Assessment of Implant Patients: Decision-making Criteria. International Journal of Oral & Maxillofacial Implants. 2001 Jan/Feb; 16(1):80-89.
10. Uysal H, Basal N. Dynamic navigation in fully edentulous maxilla. International magazine of oral implantology 2017; 3:38-41.
Contact
Dr Ricardo Henriques
Private Practice
R. S. Martinho, 423 – R/C
4505-164 Argoncilhe, Portugal
[email protected]

Magnetic Mallet y Láser de Diodo. Teórico-Práctico. 18-19 Noviembre 2022.

Aplicaciones en Odontología
-Magnetic Mallet
-Láser de diodo
Dr. Fernando Gómez-Ferrer Bolinches
Fecha: Noviembre de 2022
Viernes 18 de 15:00 a 20:00 horas
Sábado 19 de 9:30 a 19:00 horas
Modalidad:
Teórico-Práctico. Presencial.
Cupo: Limitado
Lugar: Hotel Clement Barajas
Av. General, 43
28042 Madrid
Consultas Teléfono 96.342.0478
Descripción y objetivos:
Dirigido a profesionales de la odontología que estando en posesión de las habilidades y conocimientos implantológicos convencionales deseen ampliar sus competencias con una actualización en tecnología avanzada
Programa Magnetic Mallet y EasyRoot
Teoría y práctica:
-Base científica de la tecnología Magneto Dinámica
-Función del Magnetic
-Utilidad y ventajas de uso
-Técnica expansión de cresta
-Técnica expansión de furca
-Técnica extracción de impactados
-Elevación de seno atraumática
-Cirugía guiada con el Magnetic
-Preparación de sitio de implantes
-Extracción de coronas
-Taller
-Ruegos y preguntas
Objetivos Láser de diodo
Teoría y práctica:
-Presentación
-Comprensión láser de diodo
-Ventajas y utilidades
-Funcionamiento de láser diodo K2 mobile
-Función en perio
-Endodoncia
-Ortodoncia
-Cirugía y láser, implantes
-Aftas, llagas, vestibuloplastias, mucositis
-Fotobioestimulación
-Cirugía sin anestesia
-Taller
-Ruegos y preguntas
Mira las fotos...








Te puede interesar...


Manejo de perfil de emergencia provisional inmediato. 18 Noviembre 2022.

Manejo de perfil de emergencia provisional inmediato para carga inmediata.
Diente unitario y cicatrizales personalizados.
Taller práctico.
Impartido por:
Dr. Edgar Cabrera
Dr. Jesús Ostos
Fecha: Viernes 18 de Noviembre de 2022
– 10:00 a 20:00 horas
Plazas: Limitadas a 6 asistentes
Modalidad: Presencial.
Lugar: Clínica Dental Paseo de Europa
Paseo de Europa, 12, Local 2
28703 San Sebastián de los Reyes, MADRID
Teléfono consultas: 96.342.0478
Manejo de perfil de emergencia provisional inmediato para carga inmediata.
Diente unitario y cicatrizales personalizados.
Descripción:
Un adecuado manejo de los tejidos blandos alrededor del implante antes, durante y después de los procedimientos restauradores incrementan enormemente la probabilidad de un buen resultado.
El perfil de emergencia de una restauración en un área estética presenta dos aspectos: la forma subgingival y la forma supragingival.
El manejo de de estas 2 áreas deben ser conocidos por el odontólogo cuando desea realizar una restauración con éxito.
Programa:
- Biología en tratamientos con Implantes Dentales
- Planificación Protésicamente guiada.
- Contorno crítico y subcrítico.
- Manejo de perfil de emergencia.
- ¿CUÁNDO-CÓMO-DÓNDE?.
- Manejo del sitio de extracción inmediato, temprano o tardío.
- Discusión de Casos Clínicos.
TALLER 100% PRÁCTICO SOBRE MODELOS

Gracias Dr. Armando Dias da Silva por la excelente conferencia!
MIRA LAS FOTOS...


















Te puede interesar...

Implante cónico IS-II active, hexágono interno
Inicia sesión o solicita tu usuario para ver el precio
Implante cónico IS-III active, hexágono interno
Inicia sesión o solicita tu usuario para ver el precio
Planificación 3D, Cirugía Guiada, Impresión 3D. 18-19 Noviembre 2022.
Planificación 3D. Cirugía Guiada. Impresión 3D.
Dictante: Dr. Cristian Docampo
Fecha: Noviembre de 2022
– Viernes 18 de 16:00 a 20:00 horas
– Sábado 19 de 9:30 a 18:00 horas
Modalidad: Teórico-Práctico. Presencial.
Cupo: Limitado.
Lugar:
Hospital Quirón Salud Pontevedra
Rúa Fray Juan Navarrete 9
36001 Pontevedra
Consultas Teléfono 96.342.0478
Descripción:
La odontología en estos tiempos que corren ha sufrido varios cambios importantes y debemos estar preparados para la Odontología Digital que es presente, no futuro. Para adentrarnos en ella, no hace falta pagar programas costosos ni actualizaciones de softwares que necesitan una curva de aprendizaje compleja.
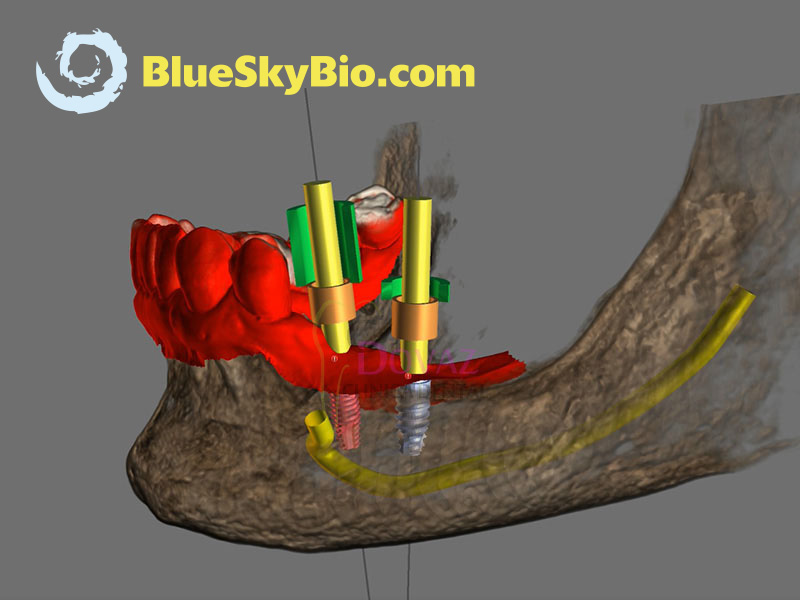
Existen muchos programas OpenSource gratuitos (BlueSkyPlan de BlueSkyBio, Autodesk Meshmixer) que nos pueden ser de gran ayuda para nuestra rutina diaria en la clínica y así, poder hacer tratamientos de calidad y convertirte en un Odontólogo Digital.
El principal objetivo del curso es que obtengas las competencias teórico-prácticas necesarias para aplicarla en clínica mediante el uso de programas sencillos y gratuitos.
Mira un vídeo...
PROGRAMA
OBJETIVOS
- Al final del curso podrás:
- Conocer toda la secuencia de manejo básico del programa BlueSkyPlan (de BlueSkyBio).
- Tomar y modificar impresiones digitales para las fases de tratamiento prequirúrgico y restaurador.
- Planificar cirugía guiada de implantes: cómo, qué, dónde.
- Planificar un diseño de guía quirúrgica utilizando el software gratuito BlueSkyPlan.
- Podrás imprimir tu propia guía.
- Saber cómo solicitar a un laboratorio la impresión 3D de tu guía quirúrgica.
TEORÍA
- Flujo de trabajo digital en odontología.
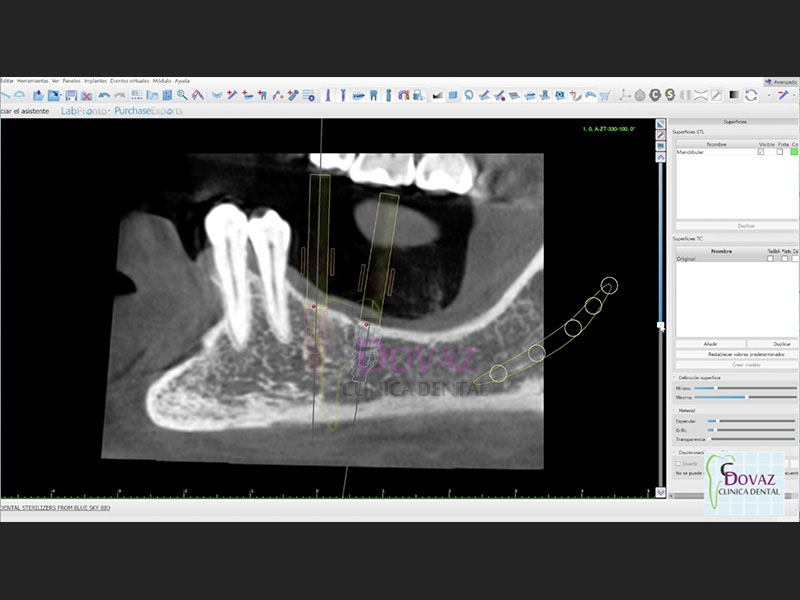
- Interpretación radiológica CBCT.
- Protocolo de escaneo TAC 3D CBCT para uso en cirugía guiada
- Diferentes sistemas de impresión 3D en odontología.
Escáner intraoral, extraoral y facial.- Técnica de escaneo óptico
- Técnica de escaneo dual.
- Ventajas y limitaciones
- Manejo de archivos digitales (STL, OBJ y DICOM).
- Toma de impresión FRI.
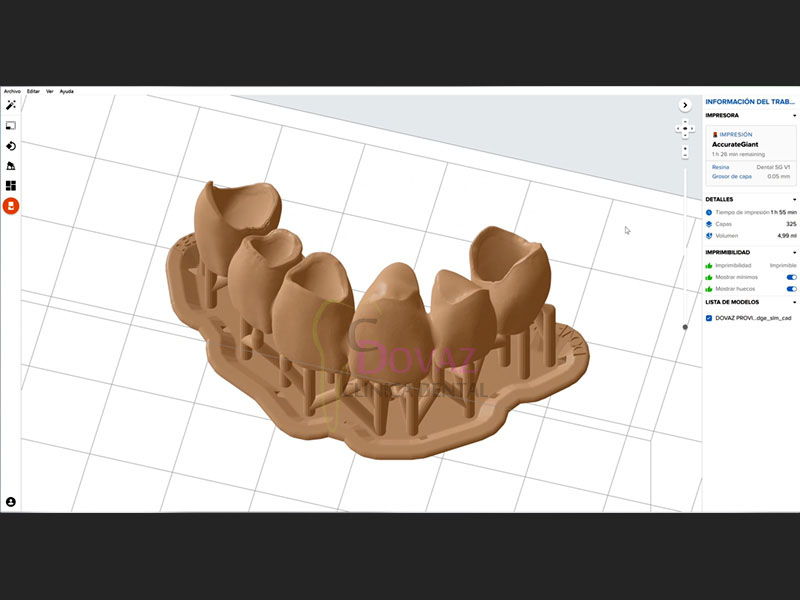
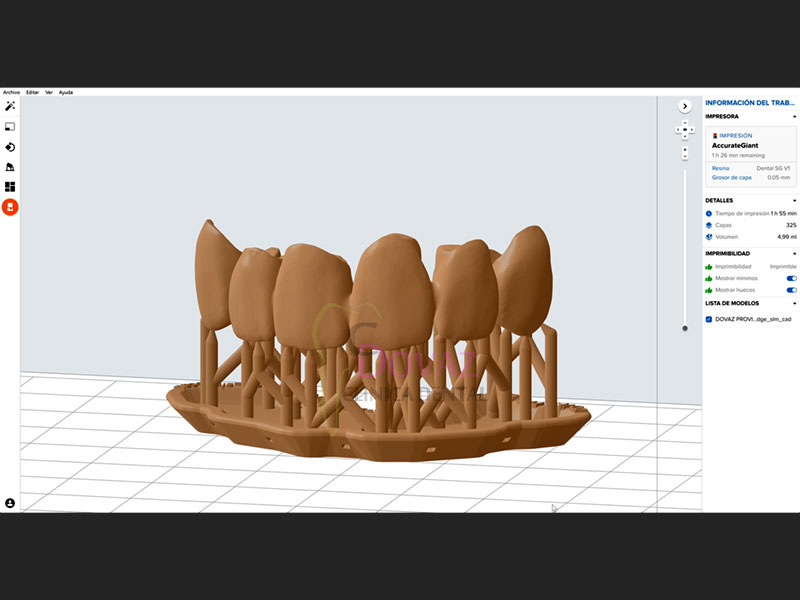
- Impresión 3D teórico-práctico. Resinas. Como imprimir correctamente.
- Funcionamiento, precauciones.
- Cirugía guiada implantológica.
- Definición
- Instrumental, kits, anillas
- Diseño de Implantes y anillas personalizadas
- Férula quirúrgica.
- Metodología para una planificación 3D en pacientes desdentados y parcialmente desdentados.
- Complicaciones de la cirugía guiada.
- Manejo del programa OpenSource BlueSkyPlan para la planificación 3D.
- Repaso del flujo de trabajo para realizar una correcta planificación.
- Protocolos para la utilización de los programas.
- Breve demostración de otros programas 3D.
PARTE PRÁCTICA
BlueSkyPlan:
- Introducción al programa.
- Importación de archivos 3D (DICOM).
- Modos de visualización
- Curva panorámica. Individualizar Nervio Dentario y Arteria Sinusal.
- Diagnóstico y planificación de implantes en base a la prótesis.
- Diseño de guía quirúrgica,
- Realización de férulas quirúrgicas.
- Exportación: qué es
- Archivos para impresión 3D
- Dientes virtuales.
- Biobigbox
MATERIAL QUE TENDRÁS QUE TRAER
Ordenador portátil con las siguientes características técnicas mínimas:
- Sistema operativo: Windows 10, 8 o 7
- Procesador Intel Core i7 o similar
- Memoria RAM de 8 a 16 GB
- Tarjeta de video NVIDIA o ATI mayor o igual a 4 GB
- Indispensable uso de ratón
- Es necesario tener ya instalados previamente el programa gratuito
Descarga en el enlace: BlueSkyPlan
ALGUNOS EJEMPLOS...
Guías quirúrgicas (cirugía guiada)

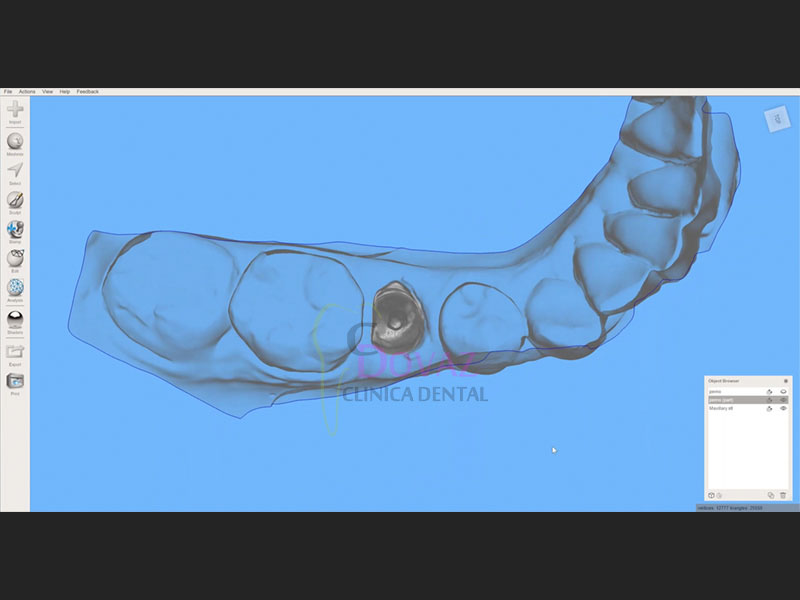
Incrustaciones Inlay/Onlay

Fabricación de provisionales

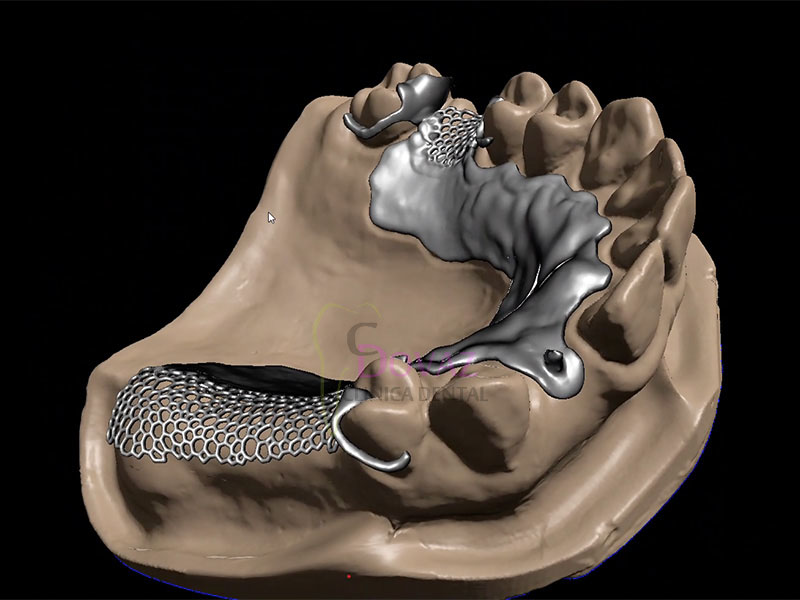
Estructuras esqueléticas

Pernos




Productos relacionados

BlueSkyPlan software para planificación
135,00 € – 3.500,00 € + IVA
Neo NaviGuide, cirugía guiada
2.800,00 € + IVA
Endodontic Microsurgery using Dynamic Navigation
Dr. Paula VIlla (Colombia, 2020)
Endodontic Microsurgery Of An Anatomically Challenging Zone Using Dynamic Navigation.
Background
Enhanced magnification and visualization, innovations in instrumentation, new sealing materials and the incorporation of soft and hard tissue augmentation practices have brought Endodontic Microsurgery (EMS) from a last resort procedure to an integral part of endodontic retreatment.1,2 The retreatment of a failing root canal treatment is fraught with potential complications. The removal of cast posts (size and length can potentiate fracture)3 distinguishing bonded fibre posts from the surrounding dentin,4 removal of separated instruments5 negotiating blocked canals,6 circumventing ledging and a myriad of other factors can complicate removal of the residual bio-load and impede resolution of periradicular pathosis.7,8. Where possible, retreatment alone would be the treatment option of choice, however, where retreatment risk factors are high, EMS is the most viable option, far more so now than prior to the transition to microsurgical protocols.
Contemporary EMS protocols provide for minimal flap size, small osteotomies and resections perpendicular to the long axis of the root. These minimally invasive practices reduce morbidity, accentuate more rapid healing, minimize the size of the retro-preparation and the number of dentinal tubuli exposed.9 Magnification and illumination have lessened the risk of damage to anatomic structures such as the IAN, maxillary sinus and the greater palatine nerve and artery. Given the inability to visualize the surgical site in three-dimensions, the possibility of procedural error remains, thus impacting on treatment options.10-13
Recently, Dynamic Navigation technology has been used in EMS to guide cutting instruments, including piezotomes, in real time, to perform osteotomies and apicoectomies. Dynamic Navigation systems map the patient’s jaws to their cbCT scan by trace registering landmarks on teeth of the jaw to be treated. The system’s stereoscopic camera recognizes optical markers attached to the jaw to be treated and the instrument to be used and monitors the drill or saw position during the surgery. Unlike static navigation guides, Dynamic Navigation procedures are not constrained to a predetermined path, there is no risk of distortion as a complication of the guide fabrication, and the inability to work in restricted areas of the mouth due to the bulk of the guide is obviated.
Dynamic navigation enables adjustment of the osteotomy pathway and the angle of the root section during the EMS procedure. The clinician follows the surgical instrument’s movement in three-dimensions on the computer monitor and assesses the surgical site through the microscope oculars. This case report presents the use of Dynamic Navigation to avoid damage to the Schneiderian membrane of the maxillary sinus while performing EMS in an anatomically challenging space.
Case Report
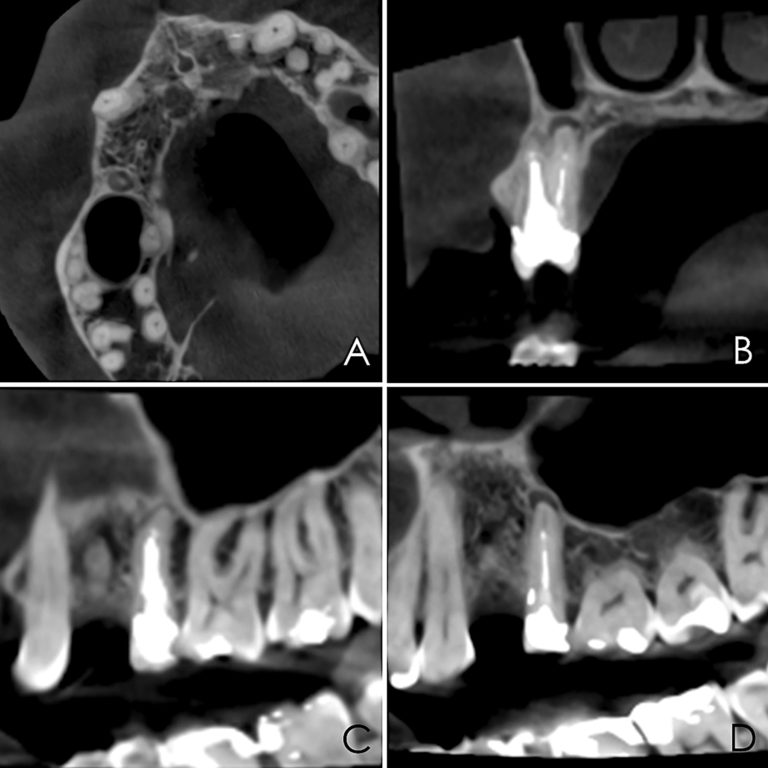
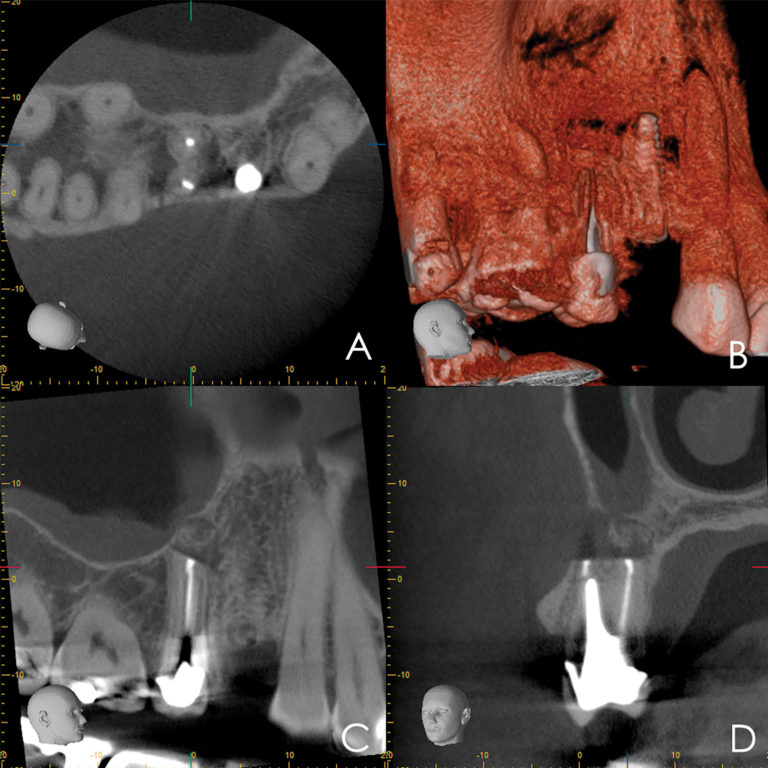
A 50-year-old male patient presented with moderate pain associated with a previously treated maxillary right second premolar (tooth #1.5). The medical history was non-contributory. The tooth had been endodontically treated and restored with a cast post/core and full crown. The patient’s scan (cbCT) revealed two separate roots, an intact buccal plate and an apical lesion associated with the palatal root (Fig 1). The tooth was moderately sensitive to vertical percussion, periodontal probe depths and mobility were within normal limits. The diagnosis was symptomatic apical periodontitis associated with a previous root canal procedure. After consultation, the patient chose to have EMS treatment done with Dynamic Navigation.
Fig 1
The proximity of the palatal root apex to the sinus floor raised the issue of an existing sinus perforation or the risk of iatrogenic creation. Dynamic Navigation enabled real-time feedback of the position of the instrument tip in a z axis as it accessed the palatal root apex and the floor of the sinus.
Lidocaine 2% with 1:80,000 epinephrine (New Stetic, Guarne, Ant. Colombia) was used to achieve profound local anesthesia and a full thickness mucoperiosteal flap with a vertical releasing incision was elevated. (Fig 2A).
Fig 2
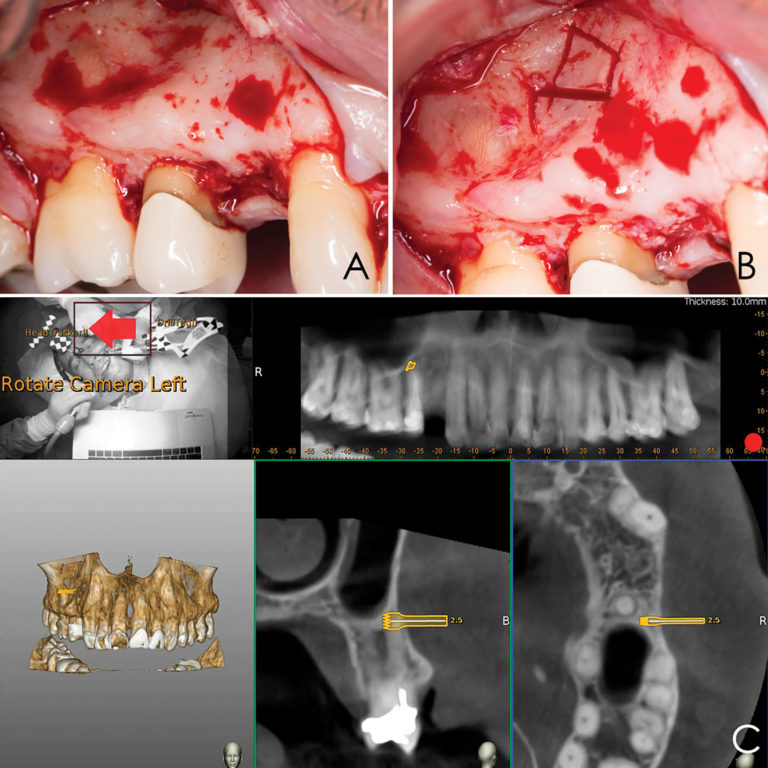
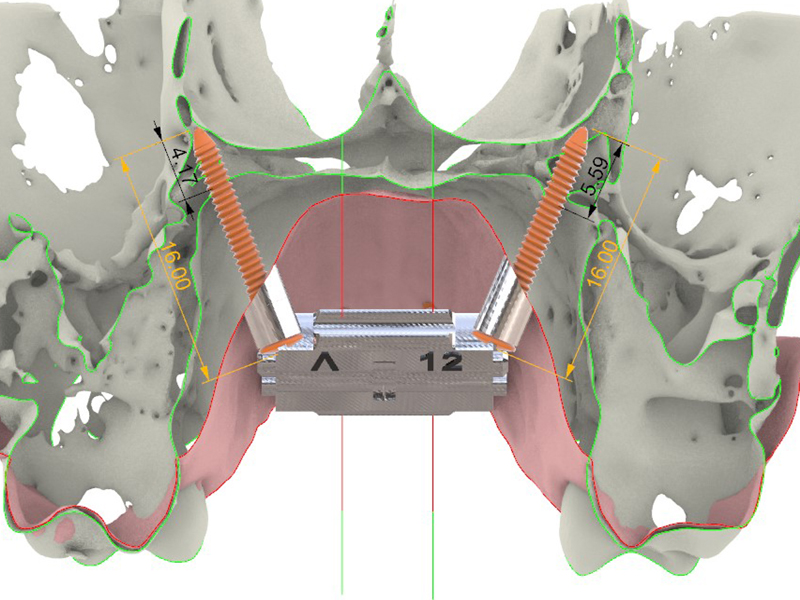
Three landmarks (up to 6 can be used) were marked on teeth displayed in the patient’s scan in a non-colinear array. A Head Tracker (optical marker) was secured to establish jaw position, a tracer tag attached to a tracer tool and a stentless trace registration of the maxilla done by creating a cloud of points around the landmarked teeth thus accurately mapping the avatar maxilla on the cbCT.
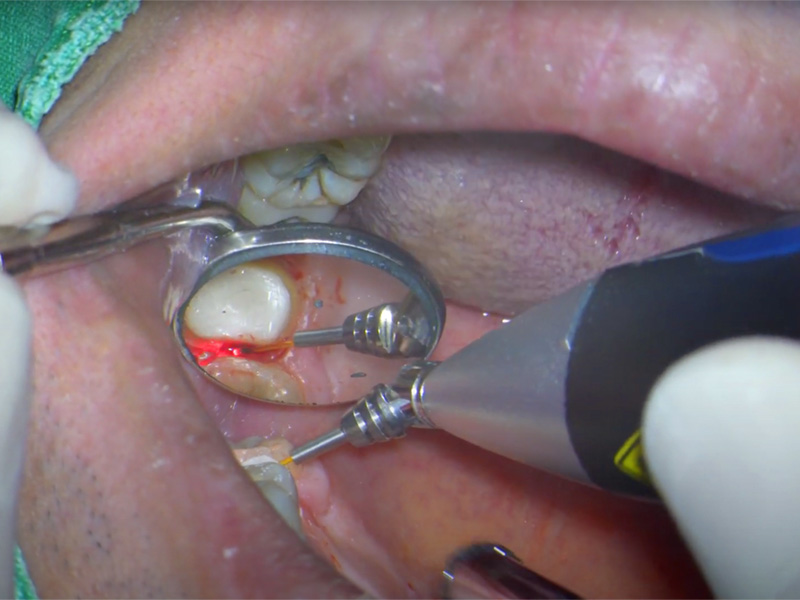
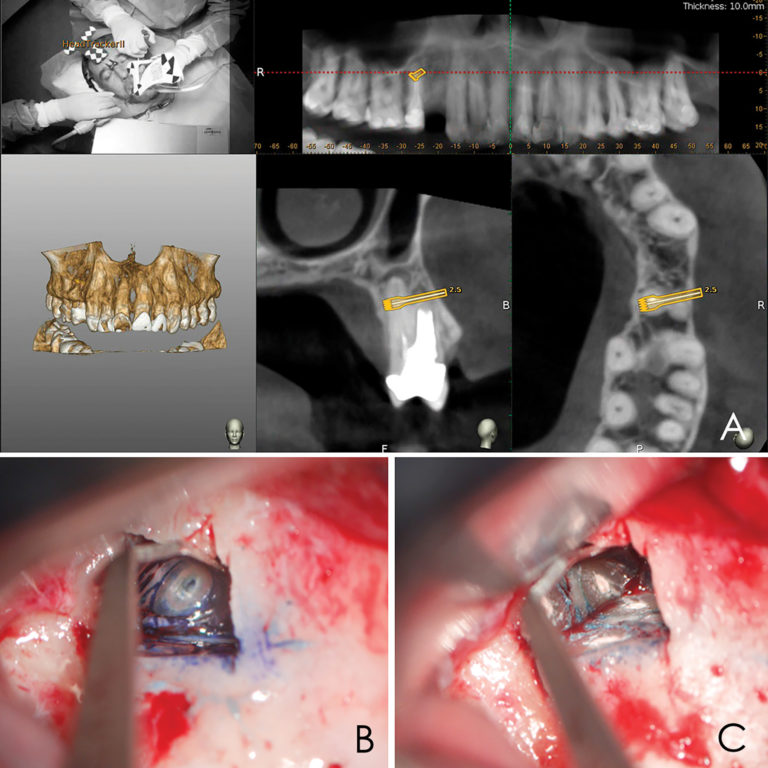
An accuracy check was performed to verify the trace registration, a drill tag (optical marker) was secured to the Piezotome® Cube handpiece (Acteon group, France) by an adapter, the LC2 saw secured to the handpiece and the saw tip calibrated. The Dynamic Navigation software algorithms enable the micron tracker (stereoscopic camera) to identify the avatar saw tip as it cuts the periphery and depth of the cortical window (Figs 2B, 2C). The position of the saw at the periphery of the palatal root resection can be precisely tracked thus preventing a sinus communication (Figs 3A, 3B). The retro-preparations were done using a E30RD ultrasonic tip (USA – NSK-Nakanishi International).
Fig 3
EndoSequence BC RRM Fast Set Putty (Brasseler, Savannah, GA) was used as the retro-sealing material (Fig 3C). Radiographs were taken to confirm the density and position of the retroseals. The post-surgical cbCT confirms the precision of the saw cuts resulting in accurate resection of both roots without complications ensuant from an iatrogenic tear of the sinus membrane (Fig 4).
Fig 4
Discussion
Dynamic Navigation has been shown to be more accurate than freehand and static navigation in surgical implant placement.14 Its effectiveness has been demonstrated for the removal of foreign objects from the maxilla and mandible, repositioning of the IAN and removal of pathology with minimal hard and soft tissue damage.15-18
Piezosurgery is a relatively new surgical technique. Its major advantages include; precision, ease of curvilinear osteotomy, less trauma to soft tissue, preservation of neurological and vascular structures, reduced hemorrhage, minimal thermal damage to the bone, and improved healing. Piezoelectric bone surgery has been demonstrated to mitigate complications during maxillary osteotomy procedures, such as oroantral communication.19-23 Vercellotti et al. introduced the piezoelectric bony window osteotomy as a simplified technique for sinus elevation24. Due to the cessation of the surgical action of the piezoelectric scalpel when it comes in contact with nonmineralized tissue, there is a reduced risk of iatrogenics25. In conjunction with Dynamic Navigation, Piezosurgery allows for the creation of a cortical window which accurately approximates the pathology about the root apices.
Conclusion
Dynamic Navigation is an exciting and promising adjunct for enhancing positive EMS outcomes in contrast to the efficacy of static navigation guides. The real-time feedback feature of Dynamic Navigation technology mitigates risk in areas close to anatomic structures. Selective and controlled osseous dissection is enhanced. The ability to alter the surgical pathway provides for an improved margin of accuracy and degree of safety. Its use in other aspects of EMS are being evaluated.
Oral Health welcomes this original article.
Photographs: Figures 1, 2, 3 Brian Waters. Figures 4-11 Sejaan Arora.
About the Authors
*Corresponding author: Prof. Paula Andrea Villa Machado, Laboratory of Immunodetection and Bioanalysis, Faculty of Dentistry, University of Antioquia. Calle 70 N° 52-21, Medellín, Colombia. Phone number: (574) 2196735 Fax: (574) 2631230. e-mail address: [email protected], [email protected].
Kenneth S. Serota has been active in online education since 1998, he is the founder of the Endodontic forum ROOTS and the interdisciplinary Facebook forum NEXUS. Dr. Serota is a clinical instructor in the University of Toronto postdoctoral endodontics department. He is the social media and marketing director for Navident Dynamic Navigation.
Dr. Felipe Restrepo is an Associate Professor at the Universidad de Antioquia teaching their postgraduate level students in endodontics and also Director of the Dental Emergencies Diploma. Dr. Restrepo has authored scientific articles in peer-reviewed journals. He can be reached at [email protected]
Navident, Navegación Dinámica con NaviBite
Dr. Cristian Docampo (Vigo)
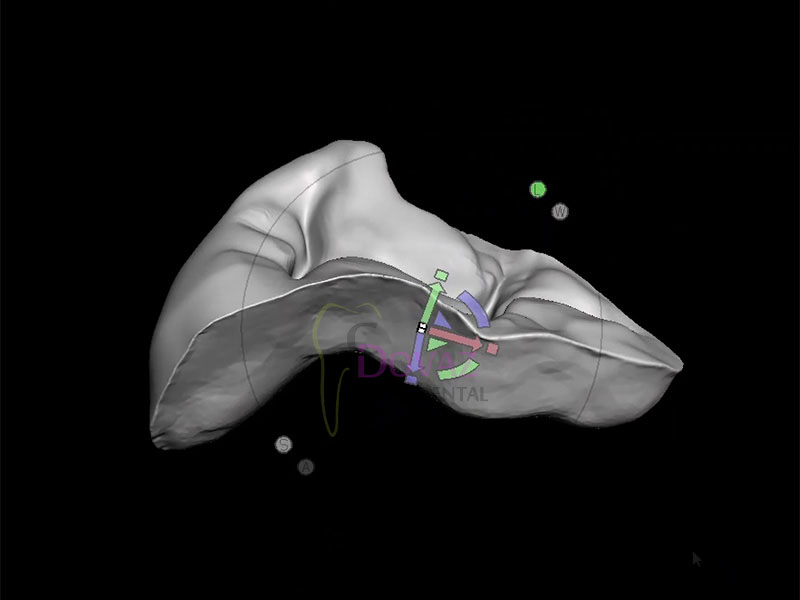
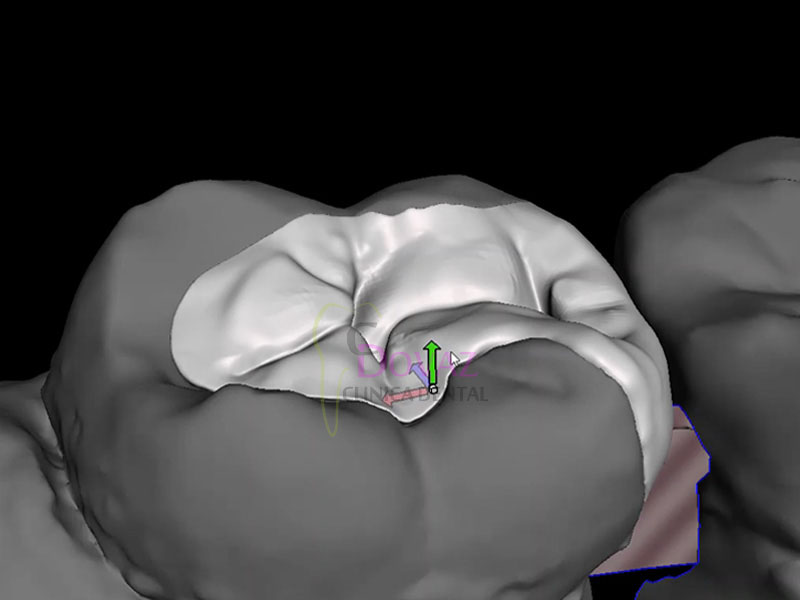
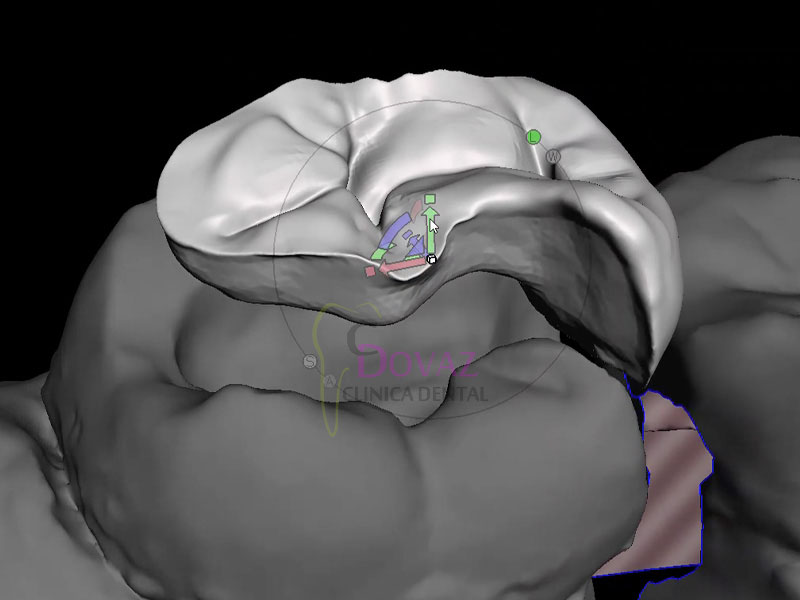
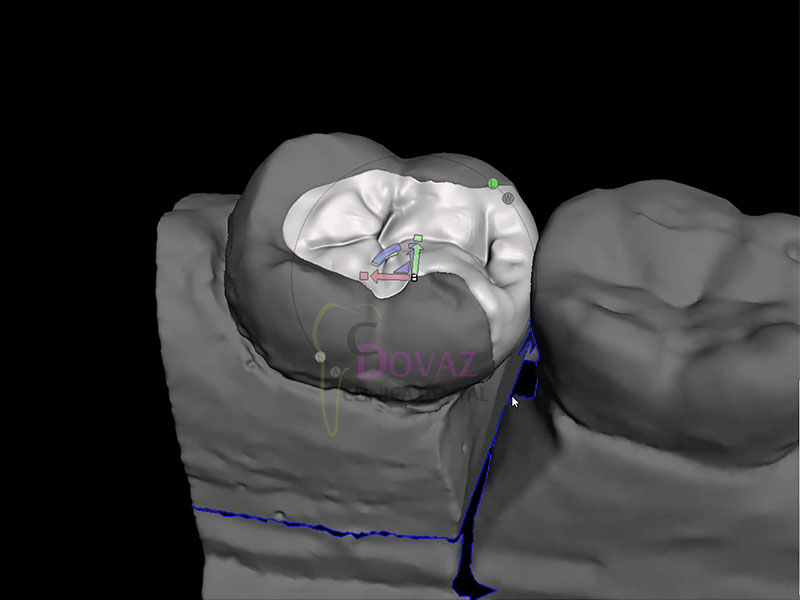
Colocación de Implantes por Navegación Dinámica
Localización con NaviBite para casos de difícil localización de puntos de referencia.
XVI Congreso SELO Burgos. Láser Odontología. 4-5 Noviembre 2022.
XVI Congreso SELO Burgos
X Reunión SELO Auxiliares e HigienistasSociedad Española de Láser y Fototerapia en Odontología
4-5 Noviembre 2022

Fecha: 4 y 5 de Noviembre de 2022
Lugar: Burgos
Congreso SELO
Sociedad Española de Láser y Fototerapia en Odontología
PROGRAMA
Viernes 4 de noviembre
PRECONGRESO
9:00-12:00 h. Curso de capacitación / Certificación para dentistas
Dr. Josep Arnabat -Dr. Toni España-Dra. María Pérez
12.00-13.00 h. Examen Certificación
CONGRESO
15.00 h. Asamblea general SELO
16.00 h. Dr. Primitivo Roig –Que la fuerza te acompañe
16.55 h. Dr. Francisco Rodríguez-Escudero –Láser en tejidos blandos y cirugía
17.50 h. Descanso / Café ExpoSELO
18.20 h. Dra. Tsira Sukhashuili –El uso del láser de diodo en endodoncia contemporánea
19.15 h. Dr. Miguel Martins –Er,Cr: YSGG Láser & Endo. Una combinación poderosa
20.05 h. Fin de Jornada
21.00 h. Cena congreso
Sábado 5 de Noviembre
9.30 h. Dr. Mario Trelles –Resurfacing labial con láser y transepidermización de medicamentos en rejuvenecimiento perioral.
10.25 h. Dr. James Carroll –Fotobiomodulación en Odontología
11.20 h. Descanso / Café en ExpoSELO
11.50 h. Dr. Christian Do Campo –El láser de diodo, mi aliado en la consulta dental
12.45 h. Dra. María Pérez –El flujo tecnológico en la práctica diaria
13.40 h. Almuerzo de trabajo en ExpoSELO
16.00 h. Mesa Redonda: Novedades Tecnológicas
17.45 h. Mesa Redonda: Tips prácticos con el láser
-Dra . Pilar Martin –Microfillers y láser en sonrisa gingival
-Dr. Daniel Abad –Alargamiento coronario sin colgajo
-Dr. Jordi Gargallo–Desinfección-descontaminación coadyuvante en cirugías orales
-Dr. Rafael Sánchez –10 razones por la que debes tener un láser en la consulta
18.50 h. Clausura en ExpoSELO
CURSO AUXILIARES E HIGIENISTAS
Sábado 5 de Noviembre
9.30 h a 11.20 h. Certificación higienistas
Dra. María Pérez-Dr. Daniel Abad-Dr. Jordi Gargallo
11.20 h. Descanso / Café en ExpoSELO
12.00 h. Dra. Pilar Martin –Salud Oral en niños y adolescentes. Aportaciones de los sistemas láser
13.40 h. Almuerzo de trabajo en ExpoSELO
16.00 h. Dr. Rubén Marzo-La higienista dental en la clínica dental moderna
17.50 h. Srta. Ana Andrés-Mantenimiento y cuidado del láser
18.30 h. Finalización del curso

MARPE-BAME. El nuevo paradigma en ortodoncia. 4 Noviembre 2022.

El nuevo paradigma de tratamiento de endognatias en adultos jóvenes con DS Xpander.
MARPE-BAME. La nueva revolución en ortodoncia.
Impartido por: Dr. Armando Dias da Silva
Fecha: Viernes 4 de Noviembre de 2022
– 9:00 a 18:00 horas
Plazas: Limitadas
Lugar: Hotel Catalonia Atocha
C/ Atocha 81
28012 Madrid
Teléfono consultas: 96.342.0478
El nuevo paradigma de tratamiento de endognatias en adultos jóvenes con DS Xpander.
Descripción:
Expansión maxilar con anclaje esquelético en adultos y jóvenes.
1. Introducción.
2. ¿Por qué usar el análisis tomográfico transversal?
3. La importancia de utilizar el análisis tomográfico Transversal.
4. El inicio…casos de MARPE paso a paso.
5. ¿Por qué cambiar de MARPE a BAME?
6. BAME: casos paso a paso, planificación, colocación y seguimiento.
7. Conclusiones.
Gracias Dr. Armando Dias da Silva por la excelente conferencia!
MIRA LAS FOTOS...
Te puede interesar...
Planificación y estructura base con DS-Xpander
620,00 € + IVA
Neobiotech World Symposium. Tailandia. 30 Octubre 2022.
Neobiotech World Symposium. 30 Octubre 2022.



Fecha: 30 Octubre 2022
Lugar:
Centara Grand & Bangkok Convention Centre at Centralworld
Bangkok, Tailandia
Hotel:
Centara Grand at CentralWorld [ver…]
999/99 Rama 1 Road
Bangkok, 10330, Thailand
Recursos Médicos te invita al Neo World Symposium:
viaje, hotel, inscripción…
Llámanos y te diremos como conseguirlo
Lista de ponentes [ver más...]

Programa [ver más...]
